LV Segmental Anatomy and Perfusion
An overview of the general segmental anatomy of the left ventricle and the associated coronary perfusion
Both ischemic and non-ischemic diseases cause focal left ventricular (LV) wall abnormalities, with ischemic being the most common. In a large study of hospital patients with abnormal left ventricular function, the PSAX papillary muscle view showed an abnormality 90% of the time, while the apical2 showed an abnormality 93% of the time. The apical4 and apical3 matched the PSAX. Thus, we need multiple LV views to assess wall motion.
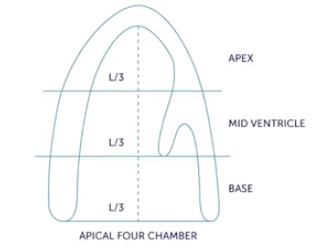
The LV is divided into three unequal regions: BASE (mitral annulus to the start of the papillary muscles), MID VENTRICLE (papillary muscles to the beginning of the distal third), and APEX (the distal third). The following image is copied from 123sonography.com.
The LV is also divided circumferentially into six regions (only four in the apex) labeled on the following frame from a basal PSAX.
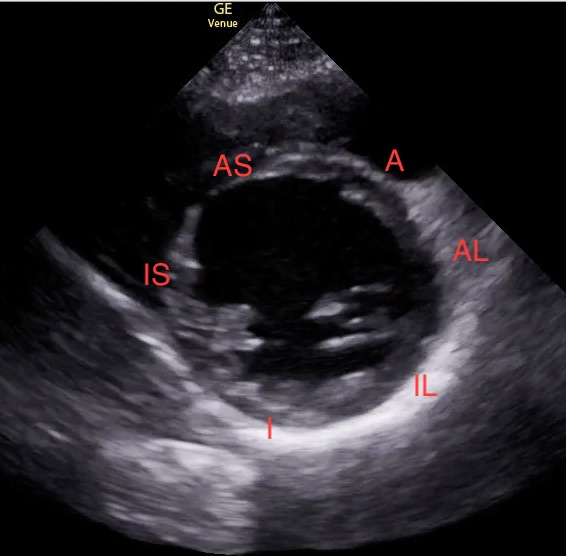
Going clockwise around the “LV doughnut,” starting at the anterior end of the IVS, are the Anterior, Anterolateral, Inferolateral, Inferior, Inferoseptal, and Anteroseptal segments. The two terminologies are combined to describe the location of a wall motion abnormality (e.g., basal inferolateral).
It is unusual for a PSAX to show all six segments clearly, as in the image above, because the lung often obscures at least part of the lateral segments. If the LV doughnut is essential in a patient with a suboptimal PSAX, an optional view called the subcostal short axis (SCSAX) can work. It is obtained from the SC4 by rotating the probe 90 degrees counterclockwise (indicator moves anterior). Slide or fan the probe to find the basal LV. This display of LV segments is rotated about 90 degrees from the PSAX. The following clip is a SCSAX showing the LV doughnut better than seen in the patient’s PSAX, although some segments are obscured by air shadow. This clip was obtained before we switched our screen indicator position to the standard cardiology convention.
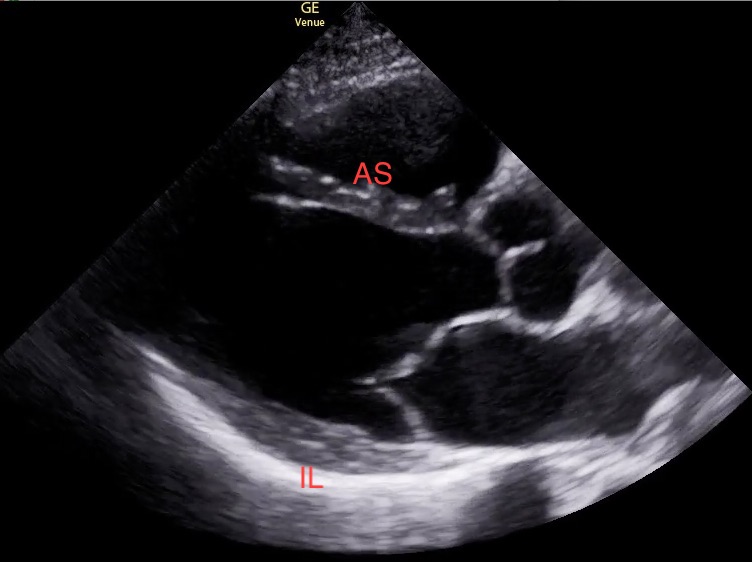
The routine PLAX of the heart is a section through the basal anteroseptal and inferolateral segments, as shown in the following image. The apical3 shows these same walls (with everything tipped up), but the apical region may be better seen.
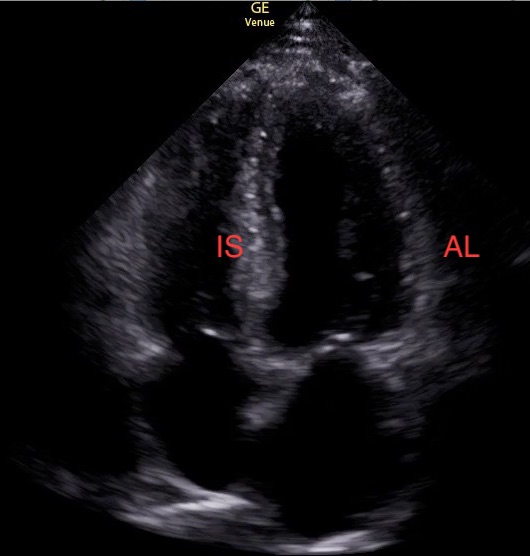
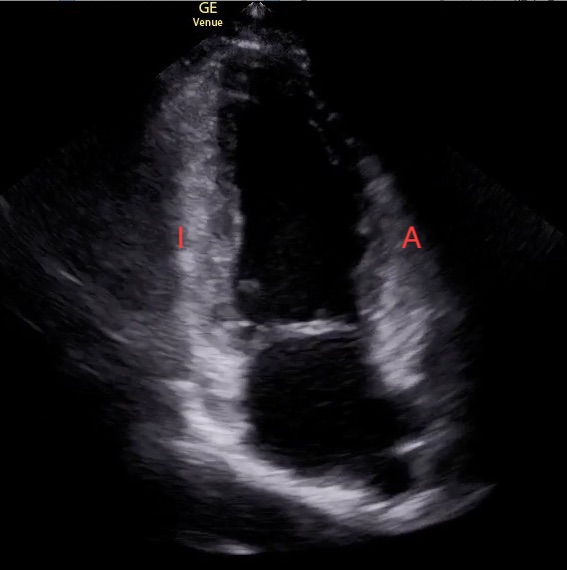
The standard apical4 shows two additional segments, the inferoseptal and the anterolateral, as shown in the following image.
The final two segments of the LV are the inferior and anterior, which are best seen with the apical2, as shown in the following image. Inhalation may sometimes improve the view of the anterior wall
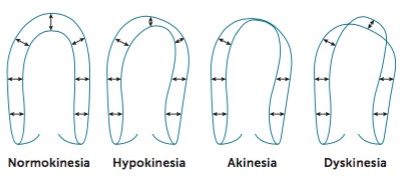
Wall motion abnormalities vary from an area that thickens less with systole and doesn’t move quite as well (hypokinesia) to more apparent abnormalities of thinned myocardium that doesn’t move at all (akinesia) and myocardium that bulges the wrong way with systole (dyskinesia). This image is from 123sonography.
When abnormal wall segments are identified, the following image identifies the coronary perfusion of the different regions of the heart. This image was taken from the American and European echocardiography societies' publication on cardiac chamber quantification in J Am Soc Echocardiogr 2015; 24:1-39.
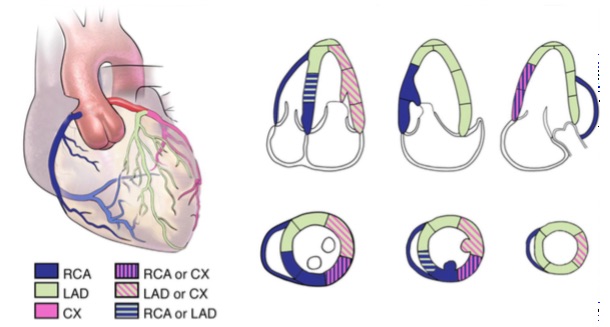
Notice that over half the heart can be perfused in two ways, so we don’t emphasize naming a culprit coronary artery.